
Stepped Care Model to Work on All that Ails the Mind (SAMWAAD) – an implementation research study addressing mental health of young people in urban informal settlements of Maharashtra, India
May 29 2026 / Posted in
An Executive Summary
Empowerment, Health and Sexuality of Adolescents (EHSAS) August, 2023
Abbreviations
| SNEHA | Society for Nutrition Education and Health Action |
| EHSAS | Empowerment Health and Sexuality of Adolescents |
| SAMWAAD | Stepped cAre Model to Work on All that Ails the MinD |
| NSW | Non-specialist Worker |
| WHO | World Health Organization |
| LMIC | Low and Middle Income Countries |
| RKSK | Rashtriya Kishor Swasthya Karyakram (National adolescent health programme) |
| AFHC | Adolescent Friendly Health Clinic |
| FGD | Focus Group Discussion |
| IDI | In-depth Interview |
| NSHW | Non-specialist Health Workers |
| M&E | Monitoring and Evaluation |
| SDQ | Strength and Difficulty Questionnaire |
| HEADSS | Home, Education, Activities/Employment, Drugs, Suicidality and Sex |
Acknowledgements:
We express our gratitude to the dedicated Non-Specialist Workers (NSWs) engaged in this study and to the young people and their parents for parting with valuable insights and information. We are grateful to Rukaiya, Shivani, Veena, Tanya and Sukaina, our dedicated team of clinical psychologists and Anjali, Aman and Onil, programme coordinators, who kept the implementing team motivated, while the SNEHA M&E team undertook most valuable quantitative analyses. We are thankful to Dr. Soumitra Pathare and Dr. Nayreen Daruwalla for guiding us with conceptualisation and to Prof. Anuradha Sovani and Dr. Ketki Ranade for reviewing the manual employed to build capacities of the NSWs. We are indebted to Vanessa D’Souza and Dr. Shanti Pantvaidya for trusting the SAMWAAD research team and for their organisational leadership. We thank the Institutional Review Board of Sigma Research and Consulting for ethical approval and the SNEHA finance and operations team for their support. We express our gratitude to Mariwala Health Initiative (MHI) and Bajaj Finserv for financial aid and to civil society partners for their insights and suggestions during consultations and meetings.
Research Team:
Seema Sharma, Vinita Ajgaonkar, Nikhat Shaikh, Sheetal Rajan, Arati Mitra, Neeta Karandikar, Keren Joy, Tanushree Das, Anu Balasubramanyam, Tanya Raj, Sujata Shirsat, Paramita Dutta & Rama Shyam
“This was the first time someone wanted to know how I feel, what I think”: A stepped care model, with Non-specialist Workers (NSWs) addressing mental health of young people in urban vulnerable communities across the Mumbai Metropolitan region
Much research for adolescent mental health in low and middle income countries have focused on non-specialist worker led counselling intervention within school and health-system platforms of care (Kumar, 2021). Literature on community based mental health interventions for young people is scanty. The SAMWAAD (dialogue/conversation in Hindi and an acronym for Stepped cAre Model to Work on All that Ails the minD) study by SNEHA was aimed at building a trans- diagnostic (Dalgleish et al. 2020)1 stepped care model to deliver psychological treatment for adolescents through Non-specialist Workers (NSWs) in urban vulnerable community settings (homes, community venues, schools, or primary health centres). In such settings, adolescents experience a range of stressors with symptoms that often cannot be ascribed to any particular disorder. A trans-diagnostic
Stepped care is effective in treating common mental disorders. Distributed along steps: less intensive treatment through self-care or lay counsellors, group therapy followed by more intensive individual based treatment by specialists and then, need based pharmacological (drug based) treatments
- (Ho Fy, et al. 2016)
approach was adopted to ensure that we do not leave behind the many young people (falling into broader diagnostic categories) in need of psychosocial support. SAMWAAD envisaged moving beyond biomedical discourses and creating community resources for mental health care accessible to young people in their own communities. It further makes way to situate pathways of treatment up to the tertiary public health services and support, within the existing ecosystem of adolescents.
Background: Making meaning of adolescent mental health
Adolescence is a formative phase of life during which patterns of growth, development, and behaviour lay a foundation for health in later life. Addressing adolescent health is crucial to breaking the intergenerational cycle of poverty and ensuring a life of well-being. This becomes an urgent priority in a country like India where every fifth person is an adolescent (Chandramouli & General, 2011) and various social determinants for mental health intersect. Depression, anxiety and behavioural disorders are among the leading causes of illness and disability, and suicide is the leading cause of mortality among young people in India (Gupta & Basera, 2021). Additionally, half of mental disorders among adults originate by the age 14 years and three fourths by 24 years (Kessler et al.,
1 Transdiagnostic approaches classify mental health problems with a focus on the quantitative structure of signs, symptoms, and behaviours associated with mental health and distress along a continua, rather than discrete categories. The risk, protective, and maintenance factors and processes implicated in mental health problems are assessed along biological, socio-environmental, or psychological boundaries rather than as specific diagnostic disorders.
2005). Estimates suggest a 7.3% (c. nine million) psychiatric morbidity and treatment gaps over 75% among 13–17-year-olds (Gaiha et al., 2020).
India is among the few low and middle-income countries with progressive legislation and a policy on mental health. India’s national adolescent health programme, Rashtriya Kishor Swasthya Karyakram (RKSK) is aimed at addressing mental health issues of young people at the community level through a network of Adolescent Friendly Health Clinics (AFHCs) located within public sub-centres (c.1 per 5000 population), primary health centres (c.1 per 30,000) and community health centres (c. 1 per 80,000). In principle, AFHCs should provide informal counselling for mental health problems and refer adolescents with severe problems to tertiary care (Ministry of Health and Family Welfare, 2014). In practice, AFHCs are scarce, mainly focused on sexual and reproductive health, and seldom used by adolescents (Barua et al., 2020).
Studies show that almost one third of the adolescents from vulnerable urban communities exhibited psychosocial issues (Sinha Roy et al., 2018). Psychological distress caused by socioeconomic adversities such as housing insecurity, overcrowding and competition for scarce amenities, exposure to and experience of violence and abuse and an absence of social networks negatively impact the mental health of residents in informal settlements. A sense of social exclusion exacerbates these risk factors (Subbaraman et al., 2014). On the other hand, mental disorder leads to educational underachievement, loss of employment, and increased health-care costs, thus perpetuating the cycle of poverty and ill health (Patel et al., 2007).
Methodology: Study design and methods
The study adopted a prospective, mixed methods design that employed both qualitative and quantitative methods. The underlying framework for this study drew upon three sources:
- The WHO Comprehensive Mental Health Action Plan 2013-30 (Kohrt et al., 2018; World Health Organization, 2021), relying on non-specialised health workers for ‘comprehensive, integrated and responsive mental health and social care services in community-based settings’
- The Friendship Bench (Chibanda et al., 2015) where trained and supervised Lay Health Workers (LHWs) adopted a task-shifting approach to provide psychosocial first aid to address common mental disorders in a community-setting, as they sat with clients on a ‘friendship bench’ and
- The Atmiyata model (Joag et al., 2020) that piloted and ran a community-based intervention with volunteers to address distress/common mental disorders among adults in rural India
A meta-analysis (Kohrt et al., 2018) on the role of communities in mental health care in LMICs, points at effective delivery of mental health interventions by non-specialists at homes, schools and refugee camps. The point of departure for this particular study was to pilot a stepped care intervention by Non-specialist Workers (NSWs) to address common mental disorders among young people (11-19 years of age) and involve their families if needed, in their own neighbourhoods.
The conceptual framework for the study depicts literature and lived experiences based mental health concerns of young people amidst poverty, social identities and discrimination, inadequate educational, infrastructure and social protection support, gender-based violence, strained relationships with parents or with friends, intimate partners and substance abuse. Not seeking help is exacerbated by lack of awareness, stigma attached to mental health terminologies and compromised access to community and institutional support. Piloting a stepped care model to assess feasibility and acceptability assumes a task shifting approach with NSWs providing psychoeducation, screening, first level counselling and referral services.
Figure 1: Conceptual Framework for the SAMWAAD Study
Defining Non-specialist Workers (NSWs): Based on a Lancet series foregrounding mental health policy in 2007, the World Health Organization (WHO), in 2008, identified ten key principles for mental health integration, beginning with the primary healthcare level, with support from Non-specialist health workers (NSHWs) - first level providers who have received general rather than specialist mental health training (Caulfield et al., 2019). This cadre includes doctors, nurses, paraprofessionals, social workers, teachers and community-level workers and does not include psychiatrists, psychologists, psychiatric nurses or mental health social workers (Van Ginneken et al., 2011). This study attempts to operationally define NSWs as follows:
Non-specialist Workers (NSWs) are a cadre of community outreach workers not specialised in mental
poverty, gender based discrimination, lack of awareness about health/socio-legal issues, to alleviate key non-medical stressors that trigger common mental disorders.
Currently, SNEHA’s Empowerment Health and Sexuality of Adolescents (EHSAS) programme caters to a cohort of approximately 4000 adolescents (10–19 years). Past programme data suggested that nearly 10-12% screen positive for mental health conditions (like dysthymia, depression, anxiety,
suicidal/self-harm thoughts amongst others) across each site and onset of mental health concerns begin by the age of 12. This implementation research, a part of the EHSAS programme, was carried out with 500 young people in three informal settlements in the Mumbai Metropolitan region.
The researchers employed both qualitative and quantitative methods of data collection. Excluding those who did not give consent, NSWs screened 413 young people for mental health concerns. Using FGDs and IDIs, evidence was gathered from 191 young people, 110 parents, 20 doctors and frontline health workers and 33 NSWs. 52 NSWs were engaged in a three-tier referral system with a) NSWs offering psychological first aid; b) clinical psychologists mentoring NSWs and addressing referral made by them and c) psychiatric referrals for severe cases. The findings from this pilot study describe four aspects: 1) young people coping with social determinants of mental health and cultural vulnerability, 2) perceptions about the SAMWAAD stepped care model – needs and benefits, 3) Non- specialist Workers (NSWs) – motivations, preparations and challenges and 4) a checklist in building and executing a community based stepped care model on adolescent mental health.
Findings from the pilot intervention involving Non-specialist workers (NSW)
- “Our children must not tread the wrong path (galat raasta)”: Young people coping with social determinants and cultural vulnerability
A pre-intervention qualitative study to understand key mental health stressors found that while adolescents experienced a range of stressors, most dealt with their issues in silence with strained parent-child communications, disrupted socialisation challenges and limited awareness about avenues to seek support and express their feelings. In the absence of specialised services beyond those offered by non-governmental organisations like SNEHA, invisibility of mental illness and related silences and stigma stood out. A noticeable lack of open discussion and acknowledgment concerning mental health stemmed from a stigmatised vocabulary with words and connotations posing the biggest barrier. Terms such as "paagalpan" (madness), "depression," "tension," "naatak" (drama) were commonly used in a derogatory manner, trivialising the significance of mental health concerns and inadvertently undermining the gravity of the subject matter.
Most young people felt that mental illness was something that “cannot be seen or understood”. They were not aware of any “doctor capable of treating such cases; the only way was to take such abnormally behaving people to a Baba (traditional healer), a dargah (shrine/mausoleum of Muslim saint with magical powers) or to others who could conduct jhaad phunk (exorcism)”. Some of them associated mental illness with “captivity in a ‘mental hospital’” to keep their “behaviour under control and avoid harming others”. Words like ‘tension’ and ‘depression’ loosely used to depict the condition of people, “who had suffered grave trauma and had withdrawn from social life, studies or livelihood, making them dependent on relatives”.
Poverty and structural inequality prevailed across all three settings in Dharavi, Kandivali and Kalwa. Most young people came from households with incomes not exceeding Rs. 15,000/- – Rs. 20,000/- (USD 180-245) per month and the families were caught up in debt traps and out of pocket expenses for health concerns. Young people here were mostly first generation learners with majority of the fathers (44%) having completed 9 to 12 years of schooling as compared to the mothers (37%) who had completed 5 to 8 years of schooling (SNEHA, 2019). Fathers worked in the informal sector as carpenters, drivers, daily wage labourers, tailors etc. Some were on contract with the Brihanmumbai Municipal Corporation. Most mothers supplemented household incomes by working as domestic helpers, cooks, tailors or by through home assignments like stitching or garland making.
Breaking the intergenerational cycle of poverty for their children was a key priority for most parents. The common refrain was that, “we have gone through poverty; our children shouldn’t go through it; we should fulfil their needs as much as we can. It can be studying, food or living” (Mother, Dharavi). This manifested in pressure to study well in most adolescents, especially boys. Many young people spoke about “tension with studies” or “tension with school and tuitions”, or “tension about what lies ahead”. The stressor related to academic performance were both external and internalised. Young people felt “afraid to write board exams after 10 years, and then again write board exams after 1 year; just hoping I do not fail.” (Adolescent boy, Kalwa). Being first-generation learners at poor quality institutions with no resources for support, young people struggled to break out of this cycle.
Most families in urban informal settlements form protective family units characterised by low communication and high expectation of conformity to social norms (Koerner & Fitzpatrick, 2006). A cultural emphasis on respecting, fearing and listening to people in ‘authority’, especially parents emerged strongly. Parents having grown up in a similar parenting culture where “fear was used to hold regard to”, or “a lot of inhibitions and respect” for their ‘elders’, expected the same of their children. The conflation of ‘feeling shame’ and ‘respect for elders’ manifested in accepted expressions of shame at one's behaviour easily transmitted across households and entire neighbourhoods.
Young people (those not feeling ashamed) had ‘loose tongue’, ‘loose morals’, or were ‘modern’ and ‘free’. There was a cultural expectation of conformity from a ‘good child’ and fear of adolescents taking the ‘galat raasta (wrong path)’. Young people ‘falling in love’, ‘answering back’ at home, ‘not listening to the elders’ or ‘roaming around’ were all those who might have chosen the ‘wrong and forbidden path’. Mothers were absolutely in disagreement with making “girlfriend and boyfriends at the age of 12-13; they are looking at the internet and doing so” (Mother, Kalwa). Parents asserted that they “are afraid of friendships as they could be bad influence.” (Mother, Dharavi).
Field level evidence suggested that parents did not explain the reason for their decisions to children. Conflicts were seen negatively, and effective conflict resolution did not happen. The material and cultural vulnerability of belonging to impoverished migrant families in urban informal settlements compelled them to conform. Our findings echoed those from a study based in Kolkata and Bangalore which emphasised that economically dependent women from urban migrant families expressed that their culture did not value women's freedom and decision‐making autonomy. This dependency promoted the stereotype among them that they were the ‘keepers’ of religious norms and practices (Das et al., 2020). Across our study sites, it emerged that these stressors spilled over, to be carried along by young people, especially young girls.
Many young people internalised their stressors and coped by pushing themselves to excel in academics and build a career, even as some took up jobs while studying. Emotional manifestations of stressors took many forms ranging from speaking openly with their friends when stressed to sharing their concerns and anxieties with their mothers or siblings and cousins. Some, however, coped by “not talking to anyone”, crying or escaping the situation by “going out when angry”. Behavioural manifestations included “breaking things” and “hitting my sister”. Though just 35% had access to smartphones, 95% young people (SNEHA, 2019) used phones as a source of recreation by engaging in Instagram, YouTube, Over the Top (OTT) platforms, PUBG, Telegram and Snapchat. Some mentioned that they used their phones for educational purposes.
“No women in our family study further or take up jobs; Aunty (NSW) has had a significant impact on my aspirations and desire to study. She helped me think about my dreams, and I felt encouraged to pursue my education. I now have a strong desire to become a teacher if given the chance.” (14-year-old girl, Dharavi)
Conflicts between parents and young people, and conflicts between siblings were often over phone usage. It emerged that phones were a source of recreation, stress and coping, assuming a nearly central position in their lives, especially owing after the COVID-19 pandemic when daily needs, education, employment, medical services etc. had become technology dependant. ‘Gaming addiction’ was the new ‘substance abuse’ now!
- “There’s at least someone whom I can talk to openly without being judged”: Perceptions about the SAMWAAD stepped care model - needs and benefits
From feelings of being ‘depressed’ to a realisation of being “hopeful about the future”, young people expressed an increased ability to feel positive, “control my anger” and be more empathetic towards people around them. Conversations with the NSWs had changed their perspectives about self-awareness and they had started working on “changing myself to change my surroundings”.
Largely, the SAMWAAD intervention seemed to have opened up spaces of communication for young people, while drawing support from their parents and it established the relevance of:
- Acceptance of the need to address emotional and mental health concerns
- The importance of listening to young people and
- The recognition of help seeking behaviour among young people
|
Area |
Total No. of Adolescents |
No. of adolescents left intervention area (1) |
Did not give Consent |
Reluctant/Time Constraint/ busy due to 10th exam (2) |
NSWs unable to reach due to location and/or time constraints (3) |
Total non- participants (1+ 2+ 3) |
Enlisted Adolescents |
| Dharavi | 200 | 9 | 10 | 4 | 7 | 30 | 170 |
|
Kandivali |
100 |
14 |
1 |
1 |
6 |
22 |
77 |
| Kalwa | 200 | 7 | 13 | 10 | 4 | 34 | 166 |
| TOTAL | 500 | 30 | 24 | 15 | 17 | 86 | 413 |
Table 1. Cumulative count of adolescents enlisted and screened (using the SDQ tool) by NSWs
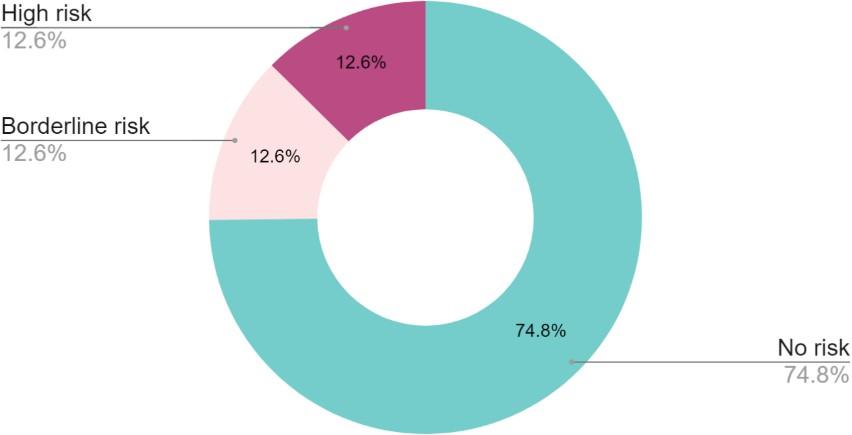
Figure 1. Prevalence distribution of High Risk, Borderline Risk and No Risk based on the SDQ screening by NSWs.
| Categories | No Risk | Borderline Risk | High Risk |
| Total Difficulty Score | 309 | 52 | 52 |
| Emotional Problem | 351 | 29 | 33 |
| Conduct Problem | 298 | 53 | 62 |
| Hyperactivity Problem | 322 | 58 | 33 |
| Peer Problem Score | 274 | 110 | 29 |
| Prosocial Score | 380 | 20 | 13 |
| Referral Data | |||
| Number of Referrals made to Clinical Psychologists | 99 | ||
| Number of Referrals made to Psychiatrists | 1 |
Table 2. Represents In-depth analysis based on scale scores on Strength and Difficulty Questionnaire (N= 413)
Prevalence of mental health concerns can be understood from total difficulty score, though intervention with adolescents were planned, based on sub-scale score and socio-cultural context. Considering the subscale score and history including abuse, grief and suicidal thoughts, those in need of intensive psychotherapy were referred to clinical psychologists. Cases that required further referral for strategic management were referred to psychiatrist.
The role of Non-specialist Workers (NSWs) was appreciated both by young people and their parents. Acceptability of a stepped care model to address mental health concerns at the community level was reinforced, especially in a resource-constrained setting such as urban informal settlements. Both adolescents and parents agreed with the need for and the benefits of “talking about feelings and emotional wellbeing” as taken up by Non-specialist Workers (NSWs) during the SAMWAAD intervention.
Shifts were seen across vocabulary and understanding of mental health. There was an evident increase in understanding and articulation of mental health, both among young people and their parents across all three locations. During the evidence gathering phase after the intervention, most young people addressed mental health using words such as ‘problem’, ‘tension’ and ‘stress’ and no longer alluded to ‘naatak (drama)’, ‘buri nazar (evil eye)’ or ‘possessed’. One young person specifically said “it is the health of the mind” and another said “brain is under pressure”. Across all interviews, an acceptability of speaking openly about these concerns was revealed.
“Someone was taking interest in me, and wanted to know what I think and feel; I had never realised that these can be important for others”, emerged as a common refrain from conversations with young people. Conversations between young people and NSWs covered a spectrum of concerns they had - academic pressure and anxieties, career aspirations, conflicts with friends, feelings of suffocation, irritation, anger and alcoholism at home. With some young people, deeper conversations on grief and abandonment took place. Parents noticed an increase in agency among young people, and their ability to draw boundaries with them in the course of the SAMWAAD intervention. Young people speaking to the NSWs under privacy was not a concern. It was insightful to note how parents’ trust towards SNEHA and their gratitude “for being with us throughout our troubles” allowed them to “leave their children completely in the safe hands of the didi and Sir (NSWs)”.
Young people had started exercising their rights and standing up to violence at home “when his father abused him, and asserted that his father must not abuse him verbally while talking to him; he had also started standing up for me, telling him that I will dial 100 and call the police if you abuse her” (mother). Regular and deeper than usual conversations with NSWs were resulting in noticeable behaviour change among young people as parents found them to be “politer and calmer” since “certain problems seemed to have been solved after these interactions”.
Beyond assisting young people through their concerns and anxieties, NSWs also seemed to have
become influencers for parents who mentioned that they were able to understand their children better
Parents found that their children were able
to renew interests in studies “after I insisted that Tai (NSW) talks to him at least once to make him understand the importance of studying rather than taking up a job; She must have been able to convince him, since now he is back to concentrating on his grade 12 studies” (Mother, Dharavi).
and had started reflecting “on my own actions; Didi helps us understand how we should be behaving before our children”. Most parents felt that while the cultural context did not allow their children to open up to their parents, “our children felt safe that they had someone they could go to, someone they trusted and was older and could guide them; the didi/sir talk to children as friends and children pour out their hearts freely”.
- Situating Non-specialist workers: Motivations, preparations and challenges
Out of the total 52 NSWs enabled to work with young people, 48 were retained for the intervention process based on convenience, availability and interest. The underpinning of the SAMWAAD stepped care model was the need for task shifting of preventive mental health care services to reach out to underserved adolescents from urban informal settlements. The assumption was that such approaches to task sharing may improve reach and effectiveness of mental health care in rural and other low-resource settings (Hoeft et al., 2018). Non-professional mental health workers have been found to have a better understanding of the community (Hunter & Riger, 1986) that stemmed from the fact that NSWs were from the same communities as their target audience and experiencing the same contexts. Almost all of them had financial constraints and the need for income generation and hence not very different from the young people and families they engaged with.
The motivation for NSWs to devote their time stemmed from their intrinsic drive to make a difference in their communities. It is worth noting that except for two or three cases, the NSWs mostly consisted of women, which aligns with the traditional gender roles prevalent. Capacity building workshops covered topics ranging from self-exploration, understanding the mental health spectrum to specific concerns of young people and practice based topics on barefoot counselling and intervention.
The NSWs expressed how their perceptions about mental health had gone through a sea change, even as they had acquired skills to address certain situations around them. They were “able to draw boundaries in their personal lives, and were learning to say ‘no’. I use more eye contact during conversations and feel more confident in holding discussions (community volunteer). The result of reduced stigma showed drastic change in self-awareness, self-care and interpersonal relationships of NSWs. While some spoke about improvement in the ways in which they had started interacting with their children and husbands, others reported personal transformations, increased confidence, improved listening skills, and the ability to identify and mediate interpersonal issues.
After completing the capacity building sessions and experiencing the intervention process, community organisers employed with SNEHA, doubling up as NSWs, mentioned that the skills
learned through SAMWAAD had allowed them to better understand and connect with young people they have been working with. The NSWs showed proficiency in identifying subtle cues and providing assistance to individuals, even those not enrolled in the programme. A wide gamut of social protection referrals arose from the intervention, such as referral for night schools for out of school adolescents and collaborating with SNEHA’s programme on Prevention of Violence against Women and Children (PVWC) to prevent child marriage. From this implementation research, emerged a framework articulated by NSWs as follows:
Figure 2. Framework emerging from NSWs’ perspective
According to clinical psychologists, NSWs’ engagement with young people resulted in “early identification, referral for moderate/severe cases and reaching a larger audience, including parents, with psychoeducation”. At the same time, critical challenges were discovered since family members of NSWs were not supportive of an ‘unpaid job’, leaving them yearning for recognition at home. Parents of young people were often suspicious owing to the stigma and ignorance around mental health; parental curiosity and lack of communal privacy, small homes with no ‘private space’ made confidentiality difficult. Some parents were hesitant to sign consent forms, expressing a deep-rooted fear of authority figures. The vulnerability of poverty stricken migrant families made them concerned about potential future obligations, alienation in “pardes - foreign land” or negative consequences “since we don’t know how our signatures might be used”! A few were not comfortable with male NSWs holding “private conversations” with their daughters.
Finally, NSWs initially doubted their performance, especially with documentation emerging as a key limitation. With mentoring support, they became more confident, comfortable, and clinical psychologists and volunteers assisted them with written articulation of cases. These challenges emphasised the need to address societal and systemic variables to support NSWs and improve mental health services for young people in their community settings.
Non-specialist Workers (NSWs) took a self-reporting assessment (Likert scale) complemented by a fidelity checklist assessment to broadly understand competency levels and areas of growth. The Likert scale showed a mean score of 77 indicating the average self- assessed fidelity across all NSWs. 35% were in the lowest tertile indicating a perception of being less effective, 38% in the middle tertile indicating a moderate effective perception of themselves and lastly 27% in the highest tertile indicating a perception of being highly effective. The expert fidelity rating, assigned by clinical psychologists showed a mean score of 65 indicating moderate competency. Qualitative analysis of fidelity ratings by supervisors found that NSWs were curious to learn and understand processes, had in-depth understanding of consent and confidentiality as crucial aspects of mental health intervention, enabled safe spaces for adolescents, efficiency with SDQ administration and identification and making appropriate referrals with respective social stressors and determinants. Also, overall there is an increase in their sensitivity and alertness with mental health and related social determinants.
- Building and executing a stepped care model on adolescent mental health: a checklist
It must be reckoned that a stepped care model involving Non-specialist Workers (NSWs) is not essentially about task replacement, but about task sharing. NSWs undertook psychoeducation as a significant preventive strategy, while identifying mental health stressors early on and making appropriate and timely referral to professionals. Clinical psychologists continued to mentor them through the processes and over time, imparted counselling and problem solving skills that enabled NSWs further while opening up more time for the specialists to address severe cases effectively. In the course of this implementation research, a few essential steps warrant enumeration:
| Key Audience | Essential Considerations and Roles |
| Mental health experts | Can build knowledge that is deep, contextual and nuanced – for a trans- diagnostic approach to social determinants of mental health |
| Implementing team | Interdisciplinary teams working on convergent adolescent programmes including gender equity, education, agency building and health access can nest meaningful mental health interventions |
| Non-specialist Workers | A combination of youth and adult NSWs work well – capacity building must be through experiential, fun pedagogies; referral pathways and self-care must be a part of the topics covered |
| Parents of young people | Psychoeducation and parenting skills must be interwoven for parents to build relationships with their children/identify stressors |
| Young people | Seeking consent is paramount; building safe spaces andconfidentiality are cornerstones; seeking their feedback is a must |
| Schools/public health system | Psychoeducation essential to build adolescent competency; Teachers, Public Health Nurses and doctors can identify stressors |
Implications for SNEHA’s mental health intervention
The SAMWAAD implementation research emphasises that stressors affecting mental health of young people often stem from social determinants, compounded by lack of awareness and stigma related to the subject. Studies cite how institutions meant to support and keep young people safe have at times been harmful, particularly to those in marginalised communities and their families (Yuen, 2019). Stepped care models like these can enable community members to create long-term support networks in underserved neighbourhoods. In the course of preparing themselves as non-specialist workers, NSWs evolved as individuals who could shed the stigma attached to ‘mental ill-health’, manage their own emotions, improve relationships within their own families and develop deeper understanding of psychosocial needs of young people at home and in their communities.
The findings from this study suggest certain recommendations for further research and implementation of community based mental health interventions:
- It is essential to hold a biopsychosocial conceptualisation for mental health and related concerns; identifying and addressing social determinants and cultural vulnerabilities can
“Person is not the problem, problem is the problem and problem is in the social”
Michael White (1988)
enhance the understanding of the needs and resources for building a mental health intervention
- A preventive and trans-diagnostic approach to mental health will help to ensure psychosocial support to the adolescents and parents who may not be having high risk or borderline mental health difficulties but are surrounded by vulnerable context
- The Strength and Difficulty Questionnaire (SDQ) must be complemented by the HEADSS screening tool to ensure a contextual understanding of young people’s mental health
- Group psychotherapy can be engaged to build safer spaces, peer support, and resilience building for emotional wellbeing; in addition, a larger audience can be catered to
- It is imperative to work on ‘parent and child alliance and communication’ – running a parenting module will help parents unlearn control and foster support for their children
- Collaborative work with the public health system to utilise Adolescent Friendly Health Clinics (AFHCs) and public schools for NSWs to provide psychosocial first aid to young people can lead to covering a larger audience in a timely manner
- Considering the urban context, living costs in Mumbai, time constraints and varied motivation of youth and older Non-specialist Workers (NSWs), SNEHA might need to think about monetary incentives to some extent, coupled with sustained non-monetary ones
Limitations
The scope of this study allowed us to engage Non-specialist Workers (NSWs) only with young people enrolled in SNEHA’s EHSAS programme. This restricted the NSWs from catering to young people beyond this cohort, thus limiting the potential of this intervention to engage with young people in their neighbourhoods who were not associated with EHSAS. As an implementation research study bound by funding cycles and a one-year-long ethical approval period, the capacity building phase of the NSWs had to be compressed over just three months before they initiated the intervention. However, they received sustained mentorship and refreshers, especially to include referral to address social determinants of mental health. Certain expectations from Non-specialist Workers (NSWs) such as following strict research protocols, taking up ‘counselling’, documenting cases were overwhelming and in the due course, we pared them down to conversations and communication with young people leading to a higher motivation among NSWs.
Though the EHSAS programme carries out psychoeducation among parents, we did not involve parents of young people in the SAMWAAD pilot intervention though we sought their consent after detailed explanations about the objectives and aims of the study. The vulnerability of urban migrant families discouraged parents from signing a written consent for the study which affected the number (though a small percentage) of young people enrolled for this study. No monetary compensation was planned for the Non-specialist Workers. Literature suggests that this aspect proves to be a barrier in implementing mental health interventions involving lay counsellors (Joag K., Pathare S. et al. 2020) and the SAMWAAD study established the same. While the NSWs associated as SNEHA employees had the time to carry out the intervention, those not employed with SNEHA found it extremely challenging to make time amidst full time jobs and household chores. It was difficult to get men to volunteer as NSWs. Both categories of NSWs remained highly motivated till the end.
Lastly, this study engaged with young people from just three urban vulnerable communities in the Mumbai Metropolitan Region and all the findings must be understood in the given contexts of these communities. We are cognisant that other such contexts might shed light on similar or divergent aspects of mental health of young people.
References:
Caulfield, A., Vatansever, D., Lambert, G., & Van Bortel, T. (2019). WHO guidance on mental health training: A systematic review of the progress for non-specialist health workers. BMJ Open, 9(1), e024059.
Chandramouli, C., & General, R. (2011). Census of india 2011. Provisional Population Totals. New Delhi: Government of India, 409–413.
Chibanda, D., Bowers, T., Verhey, R., Rusakaniko, S., Abas, M., Weiss, H. A., & Araya, R. (2015). The Friendship Bench programme: A cluster randomised controlled trial of a brief psychological intervention for common mental disorders delivered by lay health workers in Zimbabwe. Barua, A., Watson, K., Plesons, M., Chandra-Mouli, V., & Sharma, K. (2020). Adolescent health programming in India: A rapid review. Reproductive Health, 17(1), 1–10.
Das, M., Angeli, F., & van Schayck, O. C. (2020). Understanding self‐construction of health among the slum dwellers of India: A culture‐centred approach. Sociology of Health & Illness, 42(5), 1001–1023.
Dalgleish, T., Black, M., Johnston, D., & Bevan, A. (2020). Transdiagnostic approaches to mental health problems: Current status and future directions.Journal of Consulting and Clinical Psychology, 88(3), 179–195.
https://doi.org/10.1037/ccp0000482
Gaiha, S. M., Taylor Salisbury, T., Koschorke, M., Raman, U., & Petticrew, M. (2020). Stigma associated with mental health problems among young people in India: A systematic review of magnitude, manifestations and recommendations. BMC Psychiatry, 20, 1–24.
Gupta, S., & Basera, D. (2021). Youth suicide in India: A critical review and implication for the national suicide prevention policy. OMEGA-Journal of Death and Dying, 00302228211045169.
Hoeft, T. J., Fortney, J. C., Patel, V., & Unützer, J. (2018). Task‐sharing approaches to improve mental health care in rural and other low‐resource settings: A systematic review. The Journal of Rural Health, 34(1), 48– 62.
Ho FY, Yeung WF, Ng TH, Chan CS. The Efficacy and Cost-Effectiveness of Stepped Care Prevention and Treatment for Depressive and/or Anxiety Disorders: A Systematic Review and Meta-Analysis. Sci Rep. 2016 Jul 5;6:29281. doi: 10.1038/srep29281. PMID: 27377429; PMCID: PMC4932532.
Hunter, A., & Riger, S. (1986). The meaning of community in community mental health. Journal of Community Psychology, 14(1), 55–71.
Joag, K., Kalha, J., Pandit, D., Chatterjee, S., Krishnamoorthy, S., Shields-Zeeman, L., & Pathare, S. (2020). Atmiyata, a community-led intervention to address common mental disorders: Study protocol for a stepped wedge cluster randomized controlled trial in rural Gujarat, India. Trials, 21(1), 1–13.
Joag, K., Shields-Zeeman, L., Kapadia-Kundu, N., Kawade, R., Balaji, M., & Pathare, S. (2020). Feasibility and acceptability of a novel community-based mental health intervention delivered by community volunteers in Maharashtra, India: The Atmiyata programme. BMC Psychiatry, 20(1), 48. https://doi.org/10.1186/s12888-020-2466-z
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602.
Engaging Theories in Family Communication: Multiple Perspectives, 50–65.
D. R., & Patel, V. (2018). The role of communities in mental health care in low-and middle-income countries: A meta-review of components and competencies. International Journal of Environmental Research and Public Health, 15(6), 1279.
Kumar, D. (2021). School mental health program in India: need to shift from a piecemeal approach to a long- term comprehensive approach with strong intersectoral coordination. Indian J Psychiatry 63 (1): 91
Ministry of Health and Family Welfare. (2014). Strategy Handbook—Rashtriya Kishor Swasthya Karyakram.
Patel, V., Flisher, A. J., Hetrick, S., & McGorry, P. (2007). Mental health of young people: A global public-health challenge. The Lancet, 369(9569), 1302–1313.
Sinha Roy, A., Sau, M., Madhwani, K. P., Das, P., & Singh, J. K. (2018). A study on psychosocial problems among adolescents in urban slums in Kolkata, West Bengal. Int J Community Med Public Heal, 5(11), 4932.
SNEHA. (2019). EHSAS Endline survey report
Subbaraman, R., Nolan, L., Shitole, T., Sawant, K., Shitole, S., Sood, K., Nanarkar, M., Ghannam, J., Betancourt, T. S., Bloom, D. E., & Patil-Deshmukh, A. (2014). The psychological toll of slum living in Mumbai, India: A mixed methods study. Social Science & Medicine, 119, 155–169. https://doi.org/10.1016/j.socscimed.2014.08.021
Van Ginneken, N., Tharyan, P., Lewin, S., Rao, G. N., Romeo, R., & Patel, V. (2011). Non-specialist health worker interventions for mental health care in low-and middle-income countries. The Cochrane Database of Systematic Reviews, 2011(5).
White, M. (1988/89). The externalizing of the problem and the re-authoring of lives and relationships. Dulwich Centre Newsletter, Summer.
World Health Organization. (2021). Comprehensive mental health action plan 2013–2030.
Yuen, A. (2019). Pathways beyond despair. Adelaide, Australia: Dulwich Centre Publications.
Share:













